

Show Up for Yourself First
The black box is awkward at best and excruciating at worst. But it’s where change happens.
Getty/undrey
While I was researching my book I've Seen the End of You, my perspective was that of “concerned doctor with a faith conundrum.” The conundrum was, “How can I still be a good doctor for people when I can’t save them from their disease?” I had taken extensive notes in preparation for the first draft of what I thought would be my guide for helping people who were facing hard things.
But following the death of my son Mitch, I had new eyes.
Now I saw all of that trauma and tragedy—mine and my patients’—from a different point of view. I wasn’t a doctor to them now; I was a man in an equally terminal state of being, just as my glioblastoma patients, a bereaved father who knew his diagnosis would never change or be cured. And what emerged—now that I was looking with a different perspective at these people’s journeys through glioblastoma, other major neurological diseases and injuries, harsh treatments, progressive disability, and often death—was basically four stories.
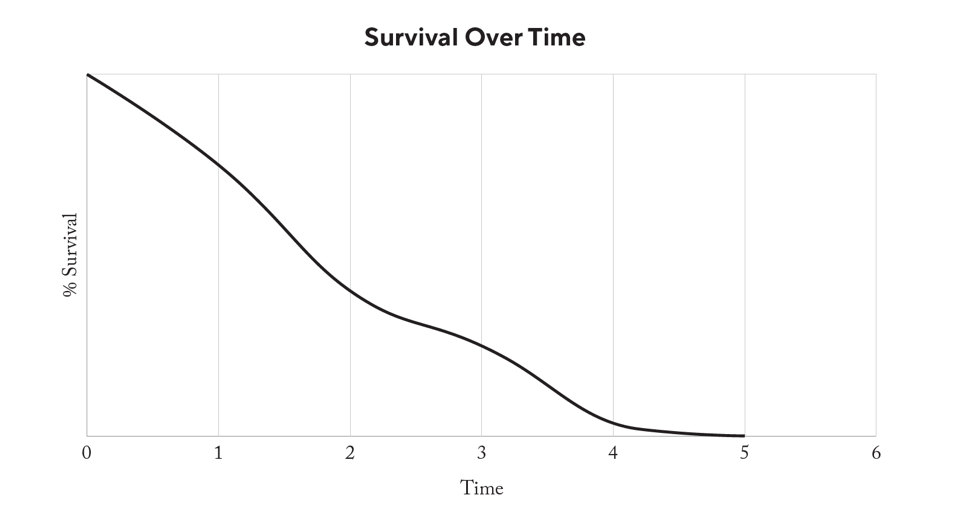
But first, a little context. When scientists look at data regarding people’s average survival rates for a particular disease, they usually chart percentage of people alive on the y-axis (vertical) and time on the x-axis (horizontal). With a malignant brain tumor like glioblastoma, the y-axis approaches zero as time passes, and by the time you get out to five years, there are very few survivors.
NOTE: The following charts are meant to show trends only and do not represent actual scientific data.
I made charts, too, although they weren’t particularly scientific, so I could visually see the trend lines of how several patients seemed to be doing in terms of their quality of life over time. I looked at the things they told me about how they were doing emotionally, how their families were, whether they felt more or less connected to God, and how happy and hopeful they felt.
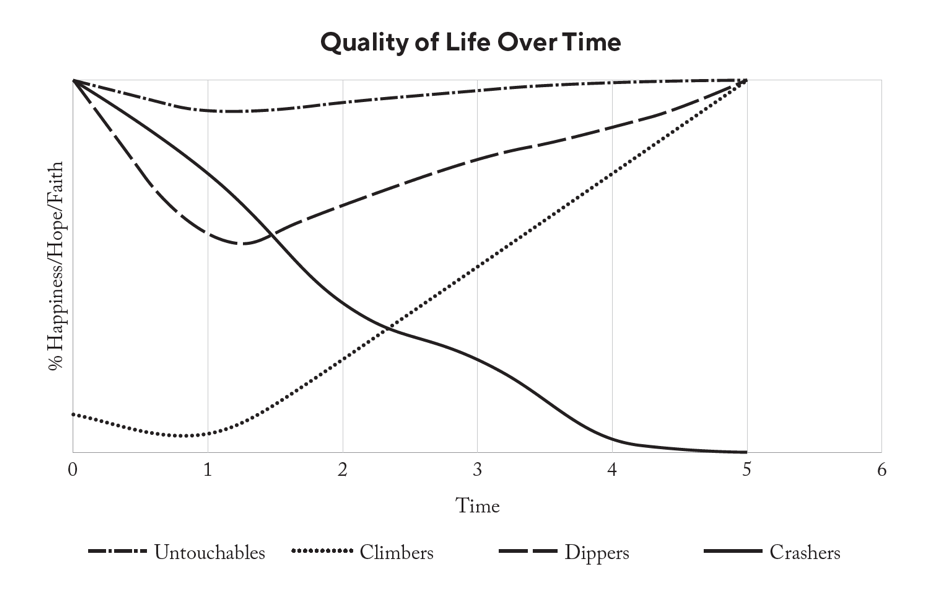
I saw four patterns over and over, which I called Crashers, Dippers, Untouchables, and Climbers. Allow me to explain the difference.
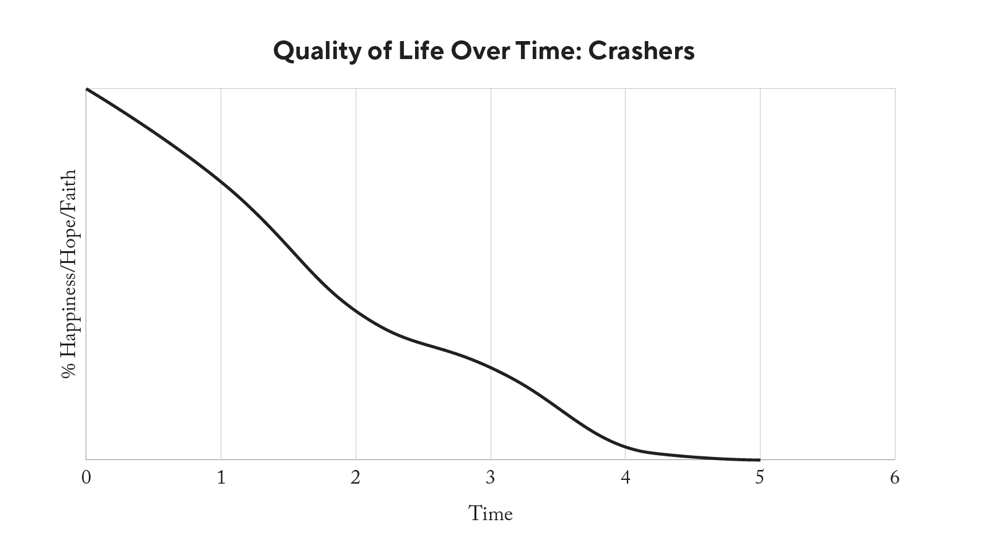
Crashers are people who seemed like they had everything together, self-reported a lot of faith, and were happy—until something bad happened, such as receiving a scary diagnosis or their loved one getting sick. These folks crashed emotionally and never recovered. What shocked me about them was that the curve looked so much like the glioblastoma survival curve; they became progressively less “alive” on the y-axis over time, even if they or their loved one survived their illness or recovered from their injury. It was as if the single problem became the defining issue of their lives.
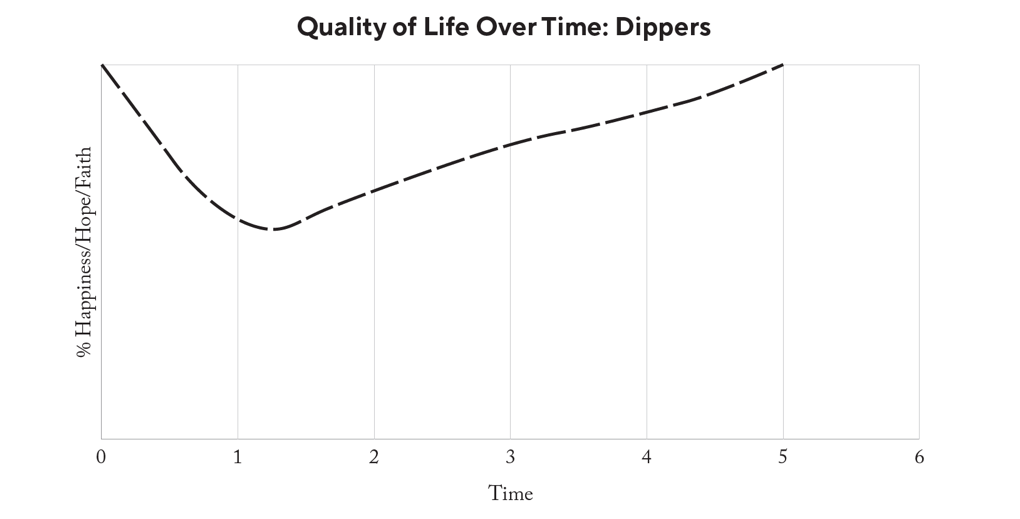
These folks started high on the y-axis with good lives and then dipped lower as they first learned of their problems. They stayed down there for a while and then somehow turned it around and began to climb, and ended up high on the quality-of-life axis regardless of their medical outcomes.
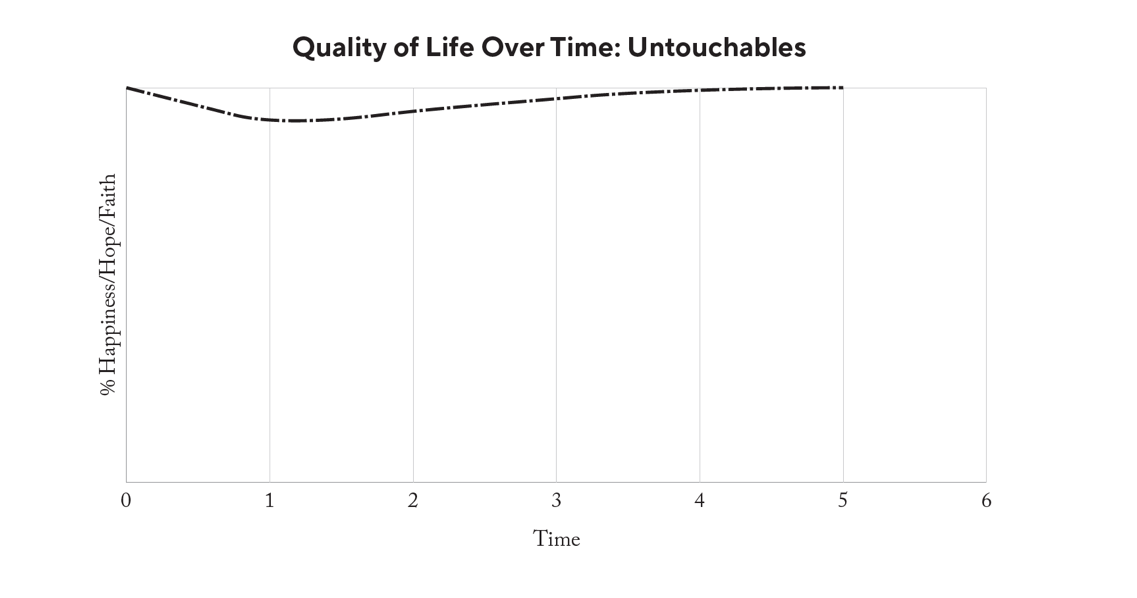
These folks seemed bulletproof. They started high, found out about their troubles, but never really wavered in their faith, their happiness, or their relationships with people or God. These patients did not experience a significant or lasting change in their baseline emotional state, even if they ultimately died of their illness.
This group surprised me the most. They started low, often with a history of trouble, addiction, prior illness, or loss. They did not report being happy or faithful or having much quality of life to begin with. When I told them they had cancer, that the injury would produce paralysis, or that their mom was not going to make it, they often received the news with something akin to having expected it. But then, somehow, something happened that caused them to discover faith, find joy, and end up being happier at the end than at the beginning.
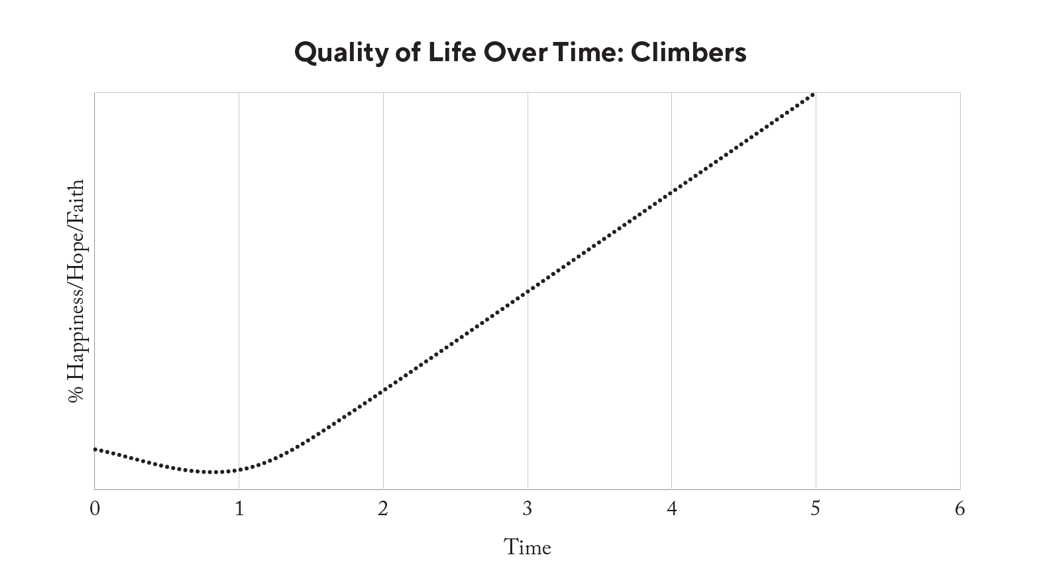
As I pored over my notes and case studies from the patients who eventually became the “characters” (real people whose names are obscured) in my book, the obvious difference in the graphs was that some people find a way to change directions and climb up the happiness/hope/faith scale—and some people don’t. Untouchables didn’t seem to need this discovery, since their curves never went down.
The Crashers, people who wound up dead inside even if their bodies lived on, never found this path back up, so their curves turned into a nearly exact copy of the glioblastoma survival graph.
Seeing the data displayed graphically made me realize the single thing I’d misunderstood from the start: The deadliest disease known to man is not glioblastoma; it is hopelessness.
This is the explanation for how some people can seem okay, but when life brings them something hard that shatters their worldview, they fall apart. I had a patient named Mr. Andrews, and his wife was the prototypical Crasher. She based her whole world on her husband being well, and when he died, she did, too, even though her body kept on living. She lost hope.
This also explains how others who believe their lives to be destined for misery feel affirmed in that thinking when they become ill, but then are shocked as people come alongside them, care and pray for them, and love them. Even in the midst of “their massive thing” (TMT), Climbers find something that makes them feel better and more hopeful than they ever did when they were well.
Climber Joey was a troubled soul, a castaway, and he found love and faith in the cancer center during the last year of his short life, which he told me was his “best year ever.” (His whole story is told in I’ve Seen the End of You). He found hope.
And the story clarifies further in people who dip and then recover. They have their faith challenged, but it turns out that the bottom holds for them, and they climb back up to being happy again, apart from their outcome. Samuel, a young man with a beautiful family, died of glioblastoma, but he finished his story strong. He found his faith to be real, and his quality of life was determined by being grateful for what he had, independent of how long he got to have it.
Untouchables, like my patient Rupert, can absorb life’s blows and not seem to flinch. Rupert had a strong faith that was not anchored on the daily circumstances of life, and he had always told his family that no matter what happened, God was enough to get him through. And when something bad actually happened, when he learned he had fatal brain cancer, he lived out what he said he believed.
I saw it so clearly: In all cases, a person’s ultimate position on the quality-of-life axis depends on their ability to separate their happiness from their circumstances. In other words, the people who manage to be okay again when they go through hard things are those who do not define being okay as having a life that is pain-free. They’re the people who can accept both of Jesus’s statements about life: It’s hard, but you can be abundantly happy anyway.
"...the people who manage to be okay again when they go through hard things are those who do not define being okay as having a life that is pain-free."
I saw all these patterns in the data, but still I knew there was more to the story of how one person hits something hard and lies down under the weight of it to wither away, while another person shrugs it off and carries on.
I realized I could not find joy again until I decided that losing my son was not going to be the only inflection point on my own quality-of-life curve. Something had to change, and that something was that I had to think about his death differently.
Just as my patients with glioblastoma were not going to survive their cancers, I was not going to wake up one morning and be magically relieved of the pain of losing Mitch or wake up and find the whole thing to have been a bad dream and that he was alive and well down the hall.
I was going to have to redefine happiness, rediscover my faith, and find a new “okay” for me. My wife, Lisa, and our other family members would have to walk that path, too, and Lisa and I would have to lead them.
It was not a matter of waiting for the pain to heal, because it wasn’t going to, at least not by itself. I was going to have to change the way I thought about it.
And I knew where we had to go: The data clearly showed that people do change their lives when they change their minds, and I had ample examples that people could do it.
I now saw a clear and efficacious treatment plan to dispense to people who were hurting, including myself as a grieving dad. And taking my own prescription was the first step toward healing.
Adapted from Hope is the First Dose by W. Lee Warren, MD. Copyright © 2023 by W. Lee Warren, MD. Published by WaterBrook, an imprint of Penguin Random House. Used with permission.
About the Author
W. Lee Warren, MD, is an award-winning author, brain surgeon, patent-holding inventor, and Iraq War veteran. He is the author of the new book Hope is the First Dose and two others: I’ve Seen the End of You—winner of the ECPA...

Get this article and many more delivered straight to your inbox weekly.




